Progressive Loading in Rehab: Part 1
- Mar 12, 2017
- 7 min read

How many times have you heard perform 3 sets of 10 repetitions for the same exercise while in your
rehabilitation? What makes this volume or work capacity special? Nothing. This is a highly generic and even naive approach to rehabilitation. There must be respect for the human stress-response and how it can produce adaptation. Clinicians today are either scared of progressive loading or, quite honestly, don't understand how it should be utilized to achieve a rehab performance goal.
Keeping this notion in mind, we must also consider who we are dealing with; as well as what tissue type is involved to effectively load them in a way that will yield a positive adaptation. Before we look at the effects of progressive loading on different soft tissue structures, we must first look at it from a global perspective. This will be the first part of a 4 part series that will allow a deeper understanding of why progressive loading is necessary during the rehab process.
Before we get into the first adaptation of this series, we need to know what is considered progressive loading. Progressive loading is a method used to improve a muscle's capacity to generate force. This can be applied using multiple methodologies: linear, non-linear, or even undulating programming. The only stipulation is that programming must allow for tissue overloading via the introduction of greater external resistance. The outcome will then be an increase in muscle force production. This is a strength gain. This is a positive adaptation.
Now let's discuss the how.
In this part we will dive into the neural adaptations that develop very early on in response to a new exercise stimulus. These neural adaptations, although necessary and essential, may be giving our patients a false positive. These patients may not be as healthy as they think and may need to either stay in therapy or transition to a training format to achieve longer lasting results.
Is this false positive the cause for so many repeat offenders? Maybe.
There are multiple neural adaptations that occur in lieu of a new physical stressor. These include motor neuron excitability, motor unit synchronization, rate coding, inhibitory inputs, as well as motor control. However these are primarily developed within the first 4-6 weeks of a stimulus. In the rehab setting, the greatest stimulus striving to generate these neural adaptations is their home exercise program. The average rehab stent for a non-surgical case is roughly 7-10 visits spread out across, you guessed it, 4-6 weeks. Thus, the chances that they are developing a long lasting or chronic strength adaptation within their rehab process is not likely. This reveals the need for the "next steps"; training or continued therapy with progressive overloading to yield longer lasting muscular adaptations, which will be discussed in a later post.

Progressive loading stresses the CNS and forces adaptation. This is how we become stronger. But why? It starts at the level of the motor neurons, of specific concern are the somatic (voluntary) motor neurons (SMN).
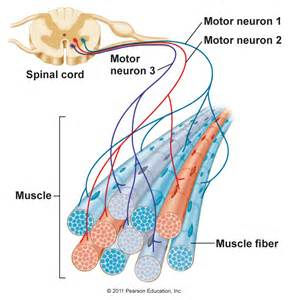
Each stimulus, or exercise, works to effectively excite SMNs. To excite these SMNs we must introduce a stimulus that will overcome the normal resting potential of a neuron. This value can be variable as each neuron is slightly unique, but it tends to hover around -60mV. Regardless, once a neuron depolarizes, the resultant is an action potential that begins a muscular contraction. Each SMN is responsible for activating a certain number of muscle fibers. This is called a motor unit, the functional unit of a muscle. Thus, the more excited SMN, the more active muscle fibers, the stronger force produced.
The important thing here is how we overcome the resting potential of the SMN because it will dictate the number of motor units activated. To achieve excitation of an SMN, it requires the presence of a neurotransmitter, acetylcholine (ACh). When our bodies become stressed, and in this case via exercise/rehabilitation exercises, our stress-response system floods the region with ACh making it easy to generate movement producing force. But what happens over time when we repeat the same movement at the same resistance? The body adapts, yes, but not in the manner we want. Our bodies are inherently lazy so instead our bodies actually work to do just the opposite of what we need them to do, in order to conserve energy. However if we are using progressive loading during exercise it forces a neural adaptation to excite more SMNs to overcome the external resistance. In order to safely achieve this feat we must improve motor unit synchronization to produce a greater muscular force.
Motor unit synchronization is the ability to recruit multiple units at one given time to increase force production. This adaptation is controlled by the CNS and occurs in response to a large physical stressor. If a muscle is not being progressively overloaded it will not develop this adaptation because there won't be a need for increased force production.
For example, what happens if a PT prescribes 3 sets of 10 straight leg raises initially and then advances this to 3 sets of 20? The small number of motor units recruited during the 3 sets of 10 may develop some muscular endurance adaptations to achieve the 20 repetitions, but there will not be any significant change in strength because there is a lack of stimulus demanding more motor units to be synchronized. Progressive loading through external resistance (ankle weights or resistance bands) or a change of exercise would achieve this and yield this neural adaptation.
This neural adaptation only carries us so far though, as muscle only has so many motor units to be recruited. This is why rate coding becomes an important neural adaptation. Rate coding is effectively how many APs are transmitted per second into a motor unit. The principle of rate coding has been shown to have an accumulation effect on muscular tension because as it increases, time allotted for SMN repolarization is reduced. Thus allowing tension to quickly build within the muscle.
So then what becomes the important aspect of rate coding?
It is the fact that it improves the rate of force development, often a strength limiting feature. As an external resistance progresses we must have the ability to overcome a larger amount of inertia. This is achieved by the rate of force development. Now some rehab specialists may say generating too much force too quickly is harmful and not desirable, but then why do we utilize Russian simulation for weak or disengaged muscles? To improve rate coding? I think so. It comes down to clinicians being fearful of loading a patient. This is hindering their results. They are stronger than you think.
This leads us into the next neural adaptation of inhibitory inputs. What the heck is that? And how does it have anything to do with progressive loading? So far we have only discussed the role of excitatory inputs, but this only have of the story. First off, inhibitory inputs can occur in a number of ways, however we will only discuss a couple all of which involve reflex loops.
When considering the role inhibitory inputs we cannot look through a myopic lens we must look peripherally and centrally. From the peripheral view, if we are increasing inhibitory input it does not mean we are forcing rest or a reduction in contraction. That would not make sense for this post. It is quite the contrary and involves inhibiting the Golgi Tendon Organs (GTO). The role of the GTO is to measure muscular tension and inhibit a muscular contraction if tension becomes too great. It achieves this through a reflexive loop. But what if we inhibit this inhibitory reflex? Math class tells us a double negative equals a positive, right? That holds true here because if we can inhibit the GTO, we can increase rate coding and the rate of force development. The resultant is an improved capacity for further progressive loading and thus strength gains.

The other area relating to inhibitory input is the basal ganglia and its' role in motor control. This is considering the central components involved. This is an overly intricate structure, but to keep it simple just know that it contains a direct loop, which produces controlled excitatory movement as well as an indirect loop striving to reduce excitatory input. Thus, while under stimulus, if we can quiet the indirect loop we may be able to improve the ability to forcefully contract a muscle.

Now this sounds nice for later in the rehab process when muscular adaptations are desired, but what about during the time sensitive interval of neural adaptation. Is their achievable benefit? Yes. Consider the role of reactive neuromuscular training (RNT). Though not directly required or designed for strength gains, RNT, aims to improve dynamic stability of joints via the principles inhibition input. This improves both movement quality and efficiency. Thus indirectly, RNT does promote strength gains and progressive loading still plays a role.
Initially, RNT, uses an external force to exaggerate a movement fault. This stimulates excitatory input to be sent to the antagonist muscle. The beauty is that this antagonistic muscle is actually the muscle aimed to be developed. It will produce a contraction to counteract the external force and increase overall stability. Now as stability is improved and we remove the external force, we are using a method of progressive loading. Once this is performed sufficiently now we can load the movement pattern and begin progressive loading as we normally would. This sets the foundation for other structural adaptations.
So in review, neural adaptations are highly crucial during the rehab process. We can achieve adaptations with regards to motor neuron excitability, motor unit synchronization, rate coding, inhibitory inputs, as well as motor control. But each of these has a ceiling effect. Note, we never discussed adaptations involving muscle, bone, or connective tissue such as ligaments/tendons or cartilage. We need adaptations within these regions too. In the upcoming posts, we will dive into each of these to gain a deeper understanding of why we progressively load a patient in rehab to achieve optimal performance.
























Comments